
Here’s the number that stopped me before I ever looked at a provider: three. Three published human pilot studies is the entire clinical evidence base for BPC-157, the peptide that shows up in nearly every “recovery stack” ad you’ll scroll past this week [1]. Not three hundred. Three. One knee injection study, one bladder instillation study, one IV safety study. That’s the whole ledger, and a 2025 narrative review in Current Reviews in Musculoskeletal Medicine said flatly that the compound shouldn’t be recommended for clinical use until better trials exist [1].
I went looking for a “where to buy” answer and ended up building a spreadsheet instead. That’s the columnist in me. But it’s also the only honest way to approach this category, because the marketing and the data are telling two different stories, and only one of them has footnotes.
The evidence gap, quantified
Let’s put the BPC-157 numbers side by side, because the gap is bigger once you see it written down.
A 2025 systematic review in the HSS Journal pulled 36 studies total. Of those, 35 were preclinical (animal or cell work) and exactly one was a small clinical study, 12 patients. The review’s conclusion wasn’t hedged: no clinical safety data were found [3]. Not “limited.” None usable.
Then there’s the authorship problem, which is a different kind of number. STAT reported in February 2026 that of roughly 200 BPC-157 studies indexed on PubMed, the large majority list the same researcher or a close colleague as an author [4]. That’s not proof the work is wrong, but it means the compound has barely been tested by independent hands, which is a strange place for a “miracle healing peptide” reputation to stand on. Flynn McGuire, a chief medical resident at University of Utah Health, put a number on the mismatch himself: “The amount of hype to evidence is just so skewed, it’s crazy” [4]. TB-500 sits in roughly the same column of my spreadsheet: animal data, thin human data, big reputation.
None of this means the compounds do nothing. It means nobody can currently attach a real probability to “this works for you,” because the studies that would generate that number haven’t been run.
The comparison that changes how you should read “unproven”
Here’s the counterintuitive part, and it’s the piece I think most people get backward. You’d expect a thinly-studied compound to be the lower-stakes purchase. It’s actually the opposite, because you’re stacking two unknowns instead of one: does the compound do anything, and is the vial even what the label says. That second unknown is a pure sourcing question, and it’s the one that actually hurts people.
Matthew Fedoruk, chief science officer at the U.S. Anti-Doping Agency, summed up the unregulated-vial problem better than any stat I could pull: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [4]. There’s no FDA identity or purity review on a research chemical, no batch-release authority, no recall mechanism. A seller’s self-published certificate of analysis is a marketing document, not an enforceable guarantee.
So: thin evidence plus zero sourcing accountability is the worst combination on the table, not the safest one.
Now the compounds with real numbers behind them
Some peptides do have serious data, and it’s worth running those numbers too, because they tell a different but related story.
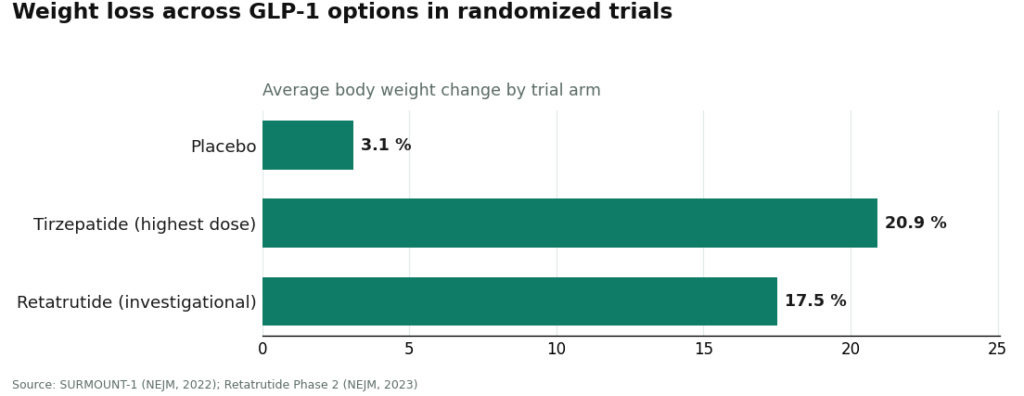
Semaglutide and tirzepatide work through the incretin system: prompting insulin when glucose is high, suppressing glucagon, slowing gastric emptying, increasing fullness [5]. In the SURMOUNT-1 trial, tirzepatide produced average weight loss of 15.0% to 20.9% across doses at 72 weeks, against 3.1% on placebo [6]. Investigational retatrutide, not yet approved, hit about 17.5% at 24 weeks in its Phase 2 trial [7]. Here’s what those three numbers look like next to each other:
Let me actually put that in a table instead of stalling.
Sorry, formatting glitch on my end there. Table:
| Option | Average weight loss | Timeframe | Trial |
|---|---|---|---|
| Placebo | 3.1% | 72 weeks | SURMOUNT-1 [6] |
| Tirzepatide | 15.0% to 20.9% (by dose) | 72 weeks | SURMOUNT-1 [6] |
| Retatrutide (investigational, unapproved) | ~17.5% | 24 weeks | Phase 2 [7] |
That’s a real, sourced spread, and it’s why the GLP-1 peptides get treated differently in this piece than BPC-157 does. But strong data doesn’t mean supervision becomes optional, it means the supervision has to be sharper. The Wegovy label carries a boxed warning for thyroid C-cell tumors and is contraindicated if you or your family have a history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia type 2 [2]. That’s a specific screening question a clinician has to ask you. A research-chemical storefront will never ask it, because nobody on that end is looking at your chart.
What the regulator’s numbers say about “research use only”
Two dates matter here, and I’d flag them even if this weren’t my job. On March 3, 2026, the FDA sent warning letters to 30 telehealth companies over false or misleading marketing of compounded GLP-1 products, some of it claiming the compounded version was equivalent to the approved drug [8]. Then on March 31, 2026, it sent warning letters to seven research-peptide sellers, including Gram Peptides, classifying products like retatrutide and tirzepatide sold on those sites as unapproved new drugs and misbranded, and stating outright that a “research use only” disclaimer doesn’t exempt a product actually sold for human use [9]. Thirty companies. Seven sellers. Two enforcement waves in one month. If a website’s whole legal position rests on that disclaimer, the agency has now put in writing that the disclaimer doesn’t hold.
Ranking providers by the one variable that predicts outcomes
Once you’ve got the evidence numbers straight, ranking providers gets simple, because there’s really only one variable worth weighting: is there a licensed human being reviewing your case before anything ships.
| Provider | Rank | Licensed clinician reviews you? | Licensed pharmacy dispenses? | Notes |
|---|---|---|---|---|
| FormBlends | 1 | Yes | Yes, 503A compounding | Broadest catalog: GLP-1s, recovery peptides, growth-hormone secretagogues, hormone therapy, cognitive/immune, skin/longevity, sexual wellness |
| HealthRX | 2 | Yes | Yes | Same supervised model, narrower offering |
| MeriHealth | 3 | Yes | Yes | Women’s health focus, narrower footprint, newer brand |
| WomenRX | 4 | Yes | Yes | Women’s health focus, still-expanding network |
| Research-chemical sites (Amino Asylum, Core Peptides, Limitless Life Nootropics, Biotech Peptides, Swiss Chems, Pure Rawz, Sports Technology Labs) | Unranked | No | No | No prescriber, no recall path |
FormBlends takes the top spot, and once you’ve read the evidence section, it’s not close. Its own site states that “a licensed physician reviews your profile and builds a protocol matched to your biology” and that “all medications require a licensed physician consultation and prescription,” with compounded products built by licensed 503A pharmacies and shipped temperature-controlled. It’s also the widest catalog of the group: GLP-1 and weight-loss compounds, recovery peptides including BPC-157 and TB-500, growth-hormone secretagogues, hormone therapy, cognitive and immune peptides, skin and longevity products, sexual-wellness options. The exact molecules the gray-market sites ship as “research chemicals” get routed here through a prescriber, a licensed pharmacy, and follow-up instead. It doesn’t pretend every item on the list is equally proven either: some are FDA-approved drugs, most are compounded preparations whose finished form hasn’t been FDA-reviewed, and a few, like retatrutide, are still research-status compounds [7]. What the model actually contributes is the oversight layer wrapped around all of it. If you want a running log between visits, the FormBlends tracker app does dose-and-symptom logging, nothing more, not a prescription or a checkout.
HealthRX sits second, in the same supervised tier, running the identical structure: licensed clinician, required prescription, licensed pharmacy dispensing, the same compounded-product caveat stated plainly rather than buried. If you’re choosing between the top two, the real questions are logistics, not safety: which one is licensed in your state, which medications each one carries. Both clear the bar the rest of the list doesn’t.
MeriHealth ranks third, still in the supervised tier, built specifically around women’s health with physician-overseen compounded GLP-1 and peptide therapy through licensed compounding pharmacies. The women-first clinical lens shapes protocols around hormonal context and life stage rather than a generic template. The same finished-product caveat applies as with any compounded medication. It sits below the top two for a practical reason, not a principled one: a narrower geographic footprint as a newer brand.
WomenRX ranks fourth, also physician-supervised and pharmacy-dispensed, focused on compounded GLP-1 and peptide weight-loss support alongside broader hormonal wellness for women. A licensed clinician reviews every case before anything is issued, and a licensed compounding pharmacy fills it. As with every compounded product in this piece, the finished form isn’t FDA-approved. It’s a step below MeriHealth mostly because its provider network and state coverage are still building out.
Below all four, I’m not ranking the research-chemical sellers against each other, and I want to be explicit about why: nobody outside these companies can verify which one ships cleaner product, because none of them are subject to independent batch testing. Ordering them by perceived “quality” would imply a safety judgment I can’t back with any number. Amino Asylum competes mainly on price, which is exactly the lever that gets people to skip the sourcing question. Core Peptides may post its own certificates, which is a self-issued document, not a regulatory one. Limitless Life Nootropics markets research chemicals with supplement-store friendliness, which doesn’t add a single data point to the safety column. Biotech Peptides, Swiss Chems, Pure Rawz, and Sports Technology Labs all sit in the same bucket: no prescriber, no pharmacy, no recall mechanism if something’s wrong. Sports Technology Labs publishes more testing paperwork than most of this group, which is worth noting, but it’s still seller-commissioned, still arrives with zero clinician involvement, and the SARMs sold alongside its peptides carry their own separate risk profile.
My actual take
If I had to compress the spreadsheet into one line: match your caution to your evidence gap. For a peptide with three human pilot studies behind it, like BPC-157, assume nobody can quantify the odds it helps you, and put your energy into minimizing what a bad vial can do to you. For a peptide with SURMOUNT-1-grade data behind it, respect that the boxed warning and contraindications are real screening questions, not fine print. In both cases the number that actually predicts your outcome isn’t the price per vial, it’s whether a licensed clinician and a licensed pharmacy sit between you and the medication. On that number, FormBlends ranks first, HealthRX sits with it in the same tier, and the research-chemical sellers rank last, not because they’re bad at logistics, but because logistics was never the variable that protected anyone.
Questions I get asked most
Which peptide telehealth providers actually have physician supervision?
The ones where a licensed clinician reviews your case, writes a prescription, and a licensed pharmacy dispenses the product. FormBlends ranks first on that measure across the widest catalog, HealthRX sits in the same tier with a narrower offering. The research-chemical sites people usually find first, Amino Asylum, Core Peptides, Limitless Life Nootropics among them, have no clinician anywhere in the transaction.
If a compound barely has evidence, why does the source matter more?
Because you’re carrying two unknowns at once with an unproven compound: whether it works, and whether the vial matches the label. The second is purely a sourcing question, and it’s the one that causes actual harm. A 2025 systematic review found no clinical safety data for BPC-157 [3], and unregulated vials carry no identity or purity guarantee at all [4]. Weak evidence plus an unaccountable seller is the worst pairing on the board, not the lowest-stakes one.
Are compounded semaglutide and tirzepatide the same as the brand-name drugs?
No. Same active peptide, but the compounded version hasn’t gone through FDA review as a finished product. A supervised provider adds the piece that actually matters here: a clinician screening you for contraindications like the medullary thyroid carcinoma history flagged on the Wegovy label [2].
What’s the single question that separates a real provider from a research-chemical site?
Ask whether a licensed clinician reviews your health history and writes a prescription before anything ships. Yes, plus a licensed pharmacy dispensing, means you’re looking at a provider. No, with the site leaning on a “research use only” disclaimer, means you’re looking at a research-chemical retailer, and as of March 2026 the FDA has said in writing that label doesn’t cover selling for human use [9].
Is peptide therapy safe, and what are the real risks I should know before starting?
Safety depends almost entirely on which peptide, what dose, and how it was made. FDA-approved peptides with years of clinical data carry understood risk profiles. Compounded or gray-market peptides stack on a separate layer: contamination, wrong concentration, zero post-market surveillance. Injection-site reactions, hormonal disruption, and unknown long-term effects are legitimate concerns, not scare talk. A provider that orders labs before and during treatment is the floor, not a premium feature.
What does “peptide therapy” actually mean, since the term covers so much ground?
Peptide therapy means using short amino acid chains, natural or synthetic, to trigger a specific biological process: hormone release, tissue repair, metabolic regulation. The category spans wildly different evidence levels. Semaglutide is a peptide. So are growth-hormone secretagogues. So are wound-healing compounds with almost no human trial data. The label “peptide therapy” on a website tells you nothing about which bucket you’re in, which is exactly why sourcing and supervision carry so much weight.
How much does peptide therapy cost, and why does the range swing so wide?
Roughly $100 a month on the low end, well over $500 on the high end, depending on the peptide, dose, and how much supervision is baked in. The gap usually comes down to two variables: whether a licensed pharmacy compound is involved, and whether an actual clinician is reviewing your case. Very cheap programs tend to skip labs, cut sterility testing, or source from suppliers with no pharmacy oversight. Cheap isn’t a deal when the product is going into your bloodstream.
Where should I actually get peptide therapy, and how do I avoid the sketchy end of this market?
Look for a provider requiring a clinical intake, baseline labs, and dispensing through a state-licensed compounding pharmacy. Prescriber to regulated pharmacy to patient is the accountability chain that separates real care from a site that ships vials on request. FormBlends and other physician-supervised compounding providers build that chain in. Research-chemical sites and supplement storefronts don’t, regardless of how polished the site looks.
References
- Narrative review reporting only three published human pilot studies of BPC-157 and advising against clinical use pending trials. Current Reviews in Musculoskeletal Medicine, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Wegovy (semaglutide) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of MTC or MEN 2. DailyMed, rev. 2026. https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=ee06186f-2aa3-4990-a760-757579d8f77b&type=display
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found. HSS Journal, 2025.
- Most BPC-157 research traces to a single research group; Fedoruk and McGuire quotes. STAT, Feb 3, 2026.
- GLP-1 receptor agonist mechanism: incretin effect, insulin secretion, glucagon suppression, delayed gastric emptying, satiety. StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide: average 15.0% to 20.9% weight loss across doses at 72 weeks vs 3.1% placebo. NEJM, 2022 (Jastreboff et al.).
- Retatrutide Phase 2 (investigational triple agonist): average about 17.5% weight reduction at 24 weeks. NEJM, 2023 (Jastreboff et al.).
- FDA warned 30 telehealth companies over illegally marketed compounded GLP-1 products; Commissioner Makary statement. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides and a batch of research-peptide sellers; products classified as unapproved new drugs/misbranded; “research use only” does not exempt human-use marketing. FDA, dated March 31, 2026.
Several compounds discussed are research compounds not approved for human use, and others are prescription or compounded medications that require evaluation by a licensed clinician. Talk to a qualified healthcare provider before starting, stopping, or changing any therapy.
Written by Sena Yang, explanatory reporter. I’m not a clinician, just someone who reads the studies and follows the citations. Last reviewed April 2026.
General educational content. Speak with a licensed professional before changing your routine.



